a.png)

About Sickle Cell Anemia
Newest Journal Articles Related:
-
Why do so many Black women die in pregnancy?
One reason: Doctors don't take them seriously (systematic discrimination against Black women who are pregnant) -
Racial Affinity Group Caucusing in Medical Education — A Key Supplement to Antiracism Curricula (the effects of structural racism in medical education in ignoring BIPOC experiences)
What Is Sickle Cell?
Sickle cell disease is an inherited genetic disorder that affects hemoglobin in red blood cells. Hemoglobin is a protein that carries oxygen to all parts of the body. With sickle cell disease, red blood cells assume a sickle shape which causes the cells to clog in the vessels. This can lead to severe pain and tissue damage.
This disease is debilitating and patients die on average in their 40s. Health care for people with SCD is barely adequate and that is another one of our many challenges.
Sickle cell disease affects millions of people throughout the world and is particularly common among those whose ancestor's came from sub-Saharan Africa; Spanish speaking regions in the Western Hemisphere (South America, the Caribbean, and Central America); Saudi Arabia; India; and Mediterranean countries such as Turkey, Greece and Italy. Americans live with sickle cell disease—a serious disease that causes sever pain, organ damage, strokes and life threatening infections—struggle to get the health care, social services and treatments they need to manage their condition.
People living with SCD have less access to comprehensive team care than people with genetic disorders such as hemophilia and cystic fibrosis. There is uneven availability and utilization of multidisciplinary specialty clinics for different genetic diseases For two disorders (ie hemophilia and cystic fibrosis), effective national networks of specialty clinics exist and reach large proportions of the taraget populations. For other disorders, notably sickle cell disease, fewer such centers are available. Models of joint management are essential to promote ongoing communications and coordination between patient and the healthcare provider particularly during the transition from pediatric care to adult care.
Sickle Cell disease FAQ's
What is hemoglobin?
Hemoglobin (Hb) is the special protein within the red blood cells that carries oxygen from the lungs to the rest of the body. Hemoglobin is what makes your blood look red in color.
Where does your hemoglobin come from?
Your hemoglobin type is inherited through family genes. The color of your hair, the color of your eyes, and your hemoglobin type are all examples of things that are determined by genes. You receive one gene for hemoglobin type from your mother and one from your father. Hemoglobin A or normal adult hemoglobin is the most common type.
What is hemoglobinopathy?
Hemoglobinopathy is a term used to describe disorders caused by the presence of abnormal hemoglobin production in the blood.
What is sickle cell trait?
Sickle cell trait occurs when a person inherits a normal hemoglobin gene (Hb A) from one parent, and a sickle hemoglobin gene (Hb S) from the other parent. This results in hemoglobin AS or sickle cell trait. A person with sickle cell trait may also be called a sickle cell carrier. Sickle cell trait is not a disease and usually does not affect one's health, but individuals with sickle cell trait can pass the sickle hemoglobin gene to their children.
How will I know if I have sickle cell trait?
A simple blood test called a hemoglobin electrophoresis will detect sickle cell trait. This test will tell if you are a carrier of the sickle cell trait or if you have the disease.
Where can I be tested for sickle cell trait?
Your physician can give you the test or the test may be obtained at some hospitals, sickle cell centers, and health department clinics.
What is sickle cell disease?
Sickle cell disease is a group of inherited blood disorders caused by the presence of hemoglobin S in red blood cells. The red cells change to a sickle (banana) shape and can clog blood vessels causing damage to the body's tissues and organs.
Sickle cell anemia (Hb SS) is the most common type of sickle cell disease. There are other hemoglobin types such as hemoglobin C or hemoglobin E, that in combination with the gene for sickle hemoglobin can result in different forms of sickle cell disease (Hb SC, Hb SE, Hb S/beta thalassemia).
What are "sickle cell conditions"?
They are sickle cell trait and the various types of sickle cell disease.
How do you get sickle cell anemia or trait?
You inherit the abnormal hemoglobin from your parents. You cannot catch it from someone else or pass it to another person like a cold or other infections. You are born with sickle cell hemoglobin and it is present for life. If you inherit only one sickle gene, you have sickle cell trait and will not develop the disease. If you inherit two sickle cell genes, you have sickle cell anemia.
How common is sickle cell anemia?
Sickle cell anemia affects millions of people throughout the world. It is particularly common among people whose ancestors come from Africa; Spanish speaking regions (South America, Cuba, Central America); Saudi Arabia; India; and Mediterranean countries, such as Turkey, Greece, and Italy. In the United States, most people who have sickle cell disease are African American. In Missouri, the disease occurs in approximately 1 in every 400 African-American births, and approximately 1 in 12 African Americans carry the sickle cell trait.
How is sickle cell anemia detected?
Most states now perform a blood test for sickle cell disease on all newborn infants. Early diagnosis of sickle cell anemia is critical so that children who have the disease can receive proper treatment. Since May 1989, all babies born in Missouri are tested for sickle cell conditions through the Missouri Newborn Screening Program (MNSP). This test is performed at the same time and from the same blood samples as other routine newborn screening tests. If the test shows the presence of sickle hemoglobin, a second blood test is performed to confirm the diagnosis. These tests also tell whether the child carries the sickle cell trait.
How is the testing done?
A small blood sample is taken from the infant's heel, usually before the baby leaves the hospital. The blood sample will show whether the baby has sickle cell trait, sickle cell disease or any other abnormal hemoglobin.
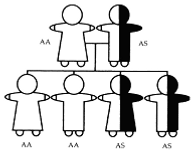
What are the chances of having a baby with sickle cell trait?
When ONE parent has sickle cell trait and the other parent has normal hemoglobin the child may inherit:
-
two normal hemoglobin genes, or
-
one normal hemoglobin gene and one sickle cell gene.
With EACH pregnancy there is a:
-
50% chance that the baby will have normal red blood cells (AA).
-
50% chance that the baby will have sickle cell trait (AS).
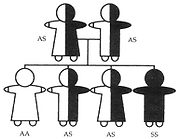
What are the chances of having a baby with sickle cell disease?
When BOTH parents have sickle cell trait (AS), the child may inherit:
-
two normal hemoglobin genes, or
-
one normal hemoglobin gene and one sickle cell gene, or
-
two sickle cell genes
With EACH pregnancy there is a:
-
25% chance that the baby's red blood cells will be normal (AA).
-
50% chance that the baby will have sickle cell trait (AS).
-
25% chance that the baby will have sickle cell disease (SS).
What medical problems are caused by sickle cell disease?
Sickle shaped red blood cells tend to get stuck in narrow blood vessels blocking the flow of blood. This can cause damage to organs including the spleen, liver and kidneys. Other complications include pain episodes, lung problems and stroke.
What should future parents know?
People who are planning to become parents should know whether they are carriers of the sickle cell gene. If they are, they may want to seek genetic counseling to find out what the chances are that their child will have sickle cell trait or sickle cell anemia.
How can I be tested?
Your doctor can do a simple blood test called a hemoglobin electrophoresis. This test will tell if you are a carrier of the sickle cell trait or if you have the disease.
-
The California Newborn Screening Program tests newborns for sickle cell and other hemoglobinopathies.
-
Family members of infants identified with sickle cell conditions can be screened at county and city health departments, family planning clinics and hospitals.
Should I have a bone marrow transplant?
-
Depends on whether or not you have a matched full sibling (you and your brother or sister have same parents). There are several studies looking at different donors for bone marrow transplant, but only a transplant from a full sibling has been studied enough to be approved by most insurance companies. If your sibling has sickle cell trait they can still be a donor.
-
There are some new therapies that have decreased the incidence of graft versus host disease (the stem cells from the donor attack the recipient of the transplant) that can cause a lot of problems including death.
-
The survival from a bone marrow transplant is very good, over 95% in some studies. The cure is less, about 85% to 90%. Which is still good.
-
Gene therapy looks very promising, but is still in the research phases.
-
Now with COVID19 studies are on hold in most cases.
-
So should you have a transplant? That is something you and your personal physician should discuss in detail. It is a decision that generally has a good outcome, but has risk.
With the new therapies available should I still be taking hydroxyurea?
-
The short answer is: Yes.
-
In studies of the new therapies some of the subjects remained on hydroxyurea and did well. It is not clear that they did better than those not taking hydroxyurea, but the studies were somewhat time limited so it is not clear how the new therapies will fair over a long period of time
-
Clearly hydroxyurea turned out to be much more effective (especially in children) than anyone thought it would in the 1980’s when it was first used for sickle cell disease. Hopefully these new therapies will also prove to be as effective as hydroxyurea.
How long should my child take penicillin?
-
Penicillin (or amoxicillin or erythromycin) was studied first in young children under 3 years old. This study was stopped early as there were deaths in the arm of the study that was randomized to the placebo compared to penicillin. Penicillin taken twice a day reduced mortality from pneumococcal infections by 95%. This was before there was a vaccine for pneumococcal disease. Even now with the vaccine, young children should be taking penicillin or erythromycin if they are allergic. Neither the vaccine nor the penicillin will be 100% effective in preventing disease as there are strains of pneumococcus that are not in the vaccine and there are infections by other bacteria that could be slowed by penicillin or other antibiotics used as prophylaxis.
-
Remember, neither treats an infection. They can slow the infection down to give you time to get medical attention.
-
Should you stop antibiotic prophylaxis? If you have S beta + thalassemia then most doctors would tell you to stop by the age of five…
How can I know if my baby will have sickle cell disease now that I am pregnant?
First know what your sickle cell status is and what your partner’s sickle cell status is.
-
If one has sickle cell trait and the other does not, then you can have a child with trait, but not with disease.
-
If you both have sickle cell trait (or are a carrier for a hemoglobin that with hemoglobin S can cause disease, like C trait) then if you both have S trait you have a 25% chance of having a child with sickle cell disease with each pregnancy
Prenatal testing for sickle cell disease can be done early.
-
You can have amniocentesis which can be diagnostic for Hemoglobinopathy like sickle cell disease (15 to 18 week’s gestation)
-
Even earlier in the pregnancy you can have Chorionic villus sampling is done 10 to 12 week’s of gestational age.
-
There are some laboratories that can test the mothers blood (a venous blood draw) for some kinds of disease (like trisomy 21, Down’s Syndrome), it is not generally available for sickle cell disease.
Avascular Necrosis
How do I know whether or not I have avascular necrosis of the hip?
Hip pain is common in people who have sickle cell disease. Most of the time it will resolve but can return. Avascular necrosis of the hip (sometimes called osteonecrosis) is permanent damage to the head of the large bone in your thigh, the femur. The head of the femur has a limited blood supply and if interrupted by vasoocclusion can cause death of the bone marrow and the bone. This can lead to collapse of the head of the femur which would then need to be replaced with surgery.
Hip pain from avascular necrosis is severe and constant over time, though it can stabilize with physical therapy, or a surgical procedure called bone decompression or sometimes “coring of the head of the femur.
If you are having hip pain and your physical examination is consistent with avascular necrosis, then either an x-ray (less sensitive) or an MRI (more sensitive) of the hip will show the degree of damage to the hip. The MRI can show that there are problems before they would show up on an x-ray or CT scan.
Depending on the results of the physical examination and the imaging a plan can be made for your therapy.
Retinopathy
How often should I have my eyes checked for sickle cell disease problems?
It is recommended the first eye check be done at the age of about 10 years and then annually thereafter. If you have an abnormal examination your doctor may have you come in more often. The eye problem in sickle cell disease is called retinopathy, which is the overgrowth of blood vessels in the eye due to vaso-occlusion of the eye vessels by sickle cell disease. These vessels are fragile and can bleed, the bleeding can cause the tissue at the back of the eye (the retina containing the sensor cells for vision) to be damaged that can lead to decreased vision or blindness if not treated.
There was a study of retinopathy in Jamaican children who had sickle cell disease that was done over 25 years. This study showed that retinopathy was five times more common in hemoglobin SC disease compared to SS disease. By the age of about 25 years, 43% of people with SC disease had retinopathy compared to 14% with SS.